Vaginal candidiasis, caused by Candida species affects a significant proportion of women worldwide. Although different antifungal medicines are being used to treat the infection, the emergence of resistance against these medicines have been reported. This study assessed the efficacy of antifungal medicines which are recommended for treatment in the Tanzania Standard Treatment Guidelines against clinical isolates of Candida spp. Presumptive Isolates of Candida spp. collected from Regional Referral Hospitals (RRH) were transported to the Tanzania Medicine and Medical Devices Authority (TMDA) Microbiology laboratory for identification and confirmation by PCR. The confirmed isolates were used for susceptibility testing to establish the efficacy of antifungal medicines. Results indicate that Candida albicans (54%) was the most prevalent Candida spp. among isolates collected. Among the antifungal medicines tested, Miconazole showed the highest efficacy against 229 isolates of Candida spp. with 89.2% of the isolates being susceptible. This was followed by Clotrimazole, with 79.9% and Nystatin, 79.5% of isolates were susceptible, while Voriconazole showed moderate efficacy with 68.9%. Fluconazole demonstrated the lowest efficacy among the tested antifungals with 63.3%. Both Candida albicans and non-albicans Candida spp. displayed similar susceptibility patterns. Out of the 229 Candida spp. isolates tested, 4.4% were found to exhibit multidrug resistance. Findings from this study suggest that despite the observed resistance, the majority of antifungal medicines listed in the Standard Treatment Guidelines in Tanzania remain effective and are still considered reliable for treating vaginal candidiasis.
| Published in | American Journal of Life Sciences (Volume 13, Issue 6) |
| DOI | 10.11648/j.ajls.20251306.13 |
| Page(s) | 198-207 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Antifungal Efficacy, Candida albicans, Vaginal Candidiasis, Antifungal Resistance, Multidrug Resistance
Hospital Name | Prevalence of Candida spp. | X2 | p - value | |
|---|---|---|---|---|
C. albicans n (%) | Non-albicans Candida spp. n (%) | |||
Amana RRH | 5 (83.3) | 1 (16.7) | 44.468 | <0.001 |
Bukoba RRH | 16 (64) | 9 (36) | ||
Dodoma RRH | 22 (66.7) | 11 (33.3) | ||
Ligula RRH | 12 (44.4) | 15 (55.6) | ||
Mawenzi RRH | 3 (42.9) | 4 (57.1) | ||
Mbeya RRH | 8 (53.3) | 7 (46.7) | ||
Mbeya Zonal | 1 (11.1) | 8 (88.9) | ||
Morogoro RRH | 19 (82.6) | 4 (17.4) | ||
Mount Meru RRH | 3 (15) | 17 (85) | ||
Mwananyamala RRH | 0 (0) | 2 (100) | ||
Sekou Toure RRH | 5 (100) | 0 (0) | ||
Singida RHH | 11 (61.1) | 7 (38.9) | ||
Sokoine RRH | 12 (35.3) | 22 (64.7) | ||
Temeke RRH | 3 (60) | 2 (40) | ||
Total | 120 (52.4) | 109 (47.6) | ||
Antifungal agent | Susceptible (S) n (%) | Intermediate (I) n (%) | Resistant (R) n (%) |
|---|---|---|---|
Miconazole (MIC) | 204 (89.19) | 11 (4.9) | 14 (6.1) |
Voriconazole (VRC) | 156 (68.9) | 4 (1.7) | 69 (30.1) |
Clotrimazole (CC) | 183 (79.9) | 16 (7) | 30 (13.1) |
Fluconazole (FLC) | 145 (63.3) | 13 (5.7) | 71 (31) |
Nystatin (NS) | 182 (79.5) | 6 (2.6) | 41(17.9) |
Drug | Susceptible n (%) | Intermediate n (%) | Resistant n (%) |
|---|---|---|---|
Miconazole | 100 (91.7) | 3 (2.8) | 6 (5.5) |
Voriconazole | 74 (67.9) | 1 (0.9) | 34 (31.2) |
Clotrimazole | 86 (78.9) | 6 (5.5) | 17 (15.6) |
Fluconazole | 68 (62.4) | 7 (6.4) | 34 (31.2) |
Nystatin | 81 (74.3) | 3 (2.8) | 25 (22.9) |
Hospital Name | MDR Status | X2 | p - value | |
|---|---|---|---|---|
MDR n (%) | Not MDR n (%) | |||
Amana RRH | 0 (0) | 6 (100) | 14.842 | 0.129 |
Bukoba RRH | 3 (12) | 22 (88) | ||
Dodoma RRH | 0 (0) | 33 (100) | ||
Ligula RRH | 4 (14.8) | 23 (85.2) | ||
Mawenzi RRH | 0 (0) | 7 (100) | ||
Mbeya RRH | 1 (6.7) | 14 (93.3) | ||
Mbeya Zonal | 0 (0) | 9 (100) | ||
Morogoro RRH | 0 (0) | 23 (100) | ||
Mount Meru RRH | 2 (10) | 18 (90) | ||
Mwananyamala RRH | 0 (0) | 2 (100) | ||
Sekou Toure RRH | 0 (0) | 5 (100) | ||
Singida RHH | 0 (0) | 18 (100) | ||
Sokoine RRH | 0 (0) | 34 (100) | ||
Temeke RRH | 0 (0) | 5 (100) | ||
Total | 10 (4.4) | 219 (95.6) | ||
ATCC | American Type Culture Collection |
CLSI | Clinical and Laboratory Standards Institute |
MDR | Multi Drug Resistance |
PCR | Polymerase Chain Reaction |
RRH | Regional Referral Hospital |
SDA | Sabouraud Dextrose Agar |
SDB | Sabouraud Dextrose Broth |
SPP | Species |
SPSS | Statistical Product and Service Solutions |
TAE | Tris-acetate-EDTA. |
TMDA | Tanzania Medicines and Medical Devices Authority |
| [1] | S. W. Kashem et al., “Candida albicans morphology and dendritic cell subsets determine T helper cell differentiation,” Immunity, vol. 42, no. 2, pp. 356–366, 2015, |
| [2] | S. S. Richter, R. P. Galask, S. A. Messer, R. J. Hollis, D. J. Diekema, and M. A. Pfaller, “Antifungal susceptibilities of Candida species causing vulvovaginitis and epidemiology of recurrent cases,” J. Clin. Microbiol., vol. 43, no. 5, pp. 2155–2162, 2005, |
| [3] | W. Lin, M. Karin, W. Lin, and M. Karin, “Review series A cytokine-mediated link between innate immunity, inflammation, and cancer,” vol. 117, no. 5, pp. 1175–1183, 2007, |
| [4] | J. M. Achkar and B. C. Fries, “Candida infections of the genitourinary tract,” Clin. Microbiol. Rev., vol. 23, no. 2, pp. 253–273, 2010, |
| [5] | D. N. Anh et al., “Prevalence, species distribution and antifungal susceptibility of Candida albicans causing vaginal discharge among symptomatic non-pregnant women of reproductive age at a tertiary care hospital, Vietnam,” BMC Infect. Dis., vol. 21, no. 1, pp. 1–10, 2021, |
| [6] | C. Chayachinda, T. Rekhawasin, M. Thamkhantho, and P. Aneklap, “Acute Vaginal Candidiasis: A review of treatment guidelines and Siriraj experience,” Thai J. Obstet. Gynaecol., vol. 29, no. 6, pp. 306–312, 2021, |
| [7] | A. O. Mohamed et al., “Prevalence of vulvovaginal candidiasis among pregnant women in Africa: A systematic review and meta-Analysis,” J. Infect. Dev. Ctries., vol. 16, no. 8, pp. 1243–1251, 2022, |
| [8] | B. Gonçalves, C. Ferreira, C. T. Alves, M. Henriques, J. Azeredo, and S. Silva, “Vulvovaginal candidiasis: Epidemiology, microbiology and risk factors,” Crit. Rev. Microbiol., vol. 42, no. 6, pp. 905–927, 2016, |
| [9] | M. F. Mushi, O. Bader, C. Bii, U. Groß, and S. E. Mshana, “Virulence and susceptibility patterns of clinical Candida spp. isolates from a tertiary hospital, Tanzania,” Med. Mycol., vol. 57, no. 5, pp. 566–572, Jul. 2019, |
| [10] | J. D. Sobel, “Recurrent vulvovaginal candidiasis,” Am. J. Obstet. Gynecol., vol. 214, no. 1, pp. 15–21, 2016, |
| [11] | J. de Cássia Orlandi Sardi et al., “Vulvovaginal Candidiasis: Epidemiology and Risk Factors, Pathogenesis, Resistance, and New Therapeutic Options,” Curr. Fungal Infect. Rep., vol. 15, no. 1, pp. 32–40, 2021, |
| [12] | Y. Shi et al., “Clinical Characteristics and Antifungal Susceptibility of Candida nivariensis from Vulvovaginal Candidiasis,” Gynecol. Obstet. Invest., vol. 85, no. 1, pp. 88–93, 2020, |
| [13] | U. Federal et al., “HHS Public Access,” vol. 4, no. 6, 2023, |
| [14] | Z. Salehei, Z. Seifi, and A. Z. Mahmoudabadi, “Sensitivity of vaginal isolates of Candida to eight antifungal drugs isolated from Ahvaz, Iran,” Jundishapur J. Microbiol., vol. 5, no. 4, pp. 574–577, 2012, |
| [15] | M. Kumar and M. Mugunthan, “Evaluation of three DNA extraction methods from fungal cultures,” Med. J. Armed Forces India, vol. 74, no. 4, pp. 333–336, 2018, |
| [16] | F. Mallus, S. Martis, C. Serra, G. Loi, T. Camboni, and A. Manzin, “Usefulness of capillary electrophoresis-based multiplex PCR assay for species-specific identification of Candida spp.,” J. Microbiol. Methods, vol. 92, no. 2, pp. 150–152, 2013, |
| [17] |
“CLSI M27M44S | Performance Standards for Antifungal Susceptibility Testing of Yeasts 3rd edition.”
https://clsi.org/standards/products/microbiology/documents/m27m44s/ |
| [18] | D. Venugopal, K. Husain, S. A. Mustafa, and S. Sabeen, “Epidemiology, risk factors and antimicrobial profile of Vulvovaginal Candidiasis (VVC): A study among women in the central region of Saudi Arabia,” J. Med. Mycol., vol. 31, no. 2, p. 101049, 2021, |
| [19] | M. F. Mushi, B. Okamo, D. C. Majinge, U. Gross, O. Bader, and S. E. Mshana, “Diversity of the diploid sequence type of Candida albicans clinical isolates from a tertiary-care hospital in Mwanza, Tanzania,” New Microbes New Infect., vol. 37, p. 100731, 2020, |
| [20] | M. F. Mushi, U. Gross, S. E. Mshana, and O. Bader, “High diversity of Candida glabrata in a tertiary hospital - Mwanza, Tanzania,” Med. Mycol., vol. 57, no. 7, pp. 914–917, 2019, |
| [21] | M. C. Fisher et al., “Tackling the emerging threat of antifungal resistance to human health,” A Alastruey-Izquierdo, J Berman, T Bicanic, EM Bignell, P Bowyer, M BromleyNature Rev. Microbiol. 2022, vol. 20, no. 9, pp. 557–571, Sep. 2022, |
| [22] | M. A. Pfaller, D. J. Diekema, J. D. Turnidge, M. Castanheira, and R. N. Jones, “Twenty Years of the SENTRY Antifungal Surveillance Program: Results for Candida Species From 1997–2016,” Acad. Pfaller, DJ Diekema, JD Turnidge, M Castanheira, RN JonesOpen forum Infect. Dis. 2019, vol. 6, no. 6, pp. S79–S94, Mar. 2019, |
| [23] | E. Boakye-Yiadom et al., “Fungal Infections, Treatment and Antifungal Resistance: The Sub-Saharan African Context,” Ther. Adv. Infect. Dis., vol. 11, pp. 1–25, 2024, |
| [24] | J. Berman, D. K.-N. R. Microbiology, and undefined 2020, “Drug resistance and tolerance in fungi,” J Berman, DJ KrysanNature Rev. Microbiol. 2020, vol. 18, no. 6, pp. 319–331, Jun. 2020, |
| [25] |
“Beyond bacteria: the growing threat of antifungal resistance,” N van Rhijn, S Arikan-Akdagli, J Beardsley, F Bongomin, A Chakrabarti, SCA Chen, T Chill. Lancet, 2024, Accessed: Sep. 24, 2025. Available:
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(24)01695-7/abstract |
| [26] | N. W.-I. and drug resistance and undefined 2017, “Antifungal resistance: current trends and future strategies to combat,” Taylor Fr. WiederholdInfection drug Resist. 2017•Taylor Fr., vol. 10, pp. 249–259, Aug. 2017, |
| [27] |
N. Robbins, L. C.-C. Biology, and undefined 2021, “Antifungal drug resistance: Deciphering the mechanisms governing multidrug resistance in the fungal pathogen Candida glabrata,” N Robbins, LE CowenCurrent Biol. 2021, Accessed: Sep. 24, 2025. Available:
https://www.cell.com/current-biology/fulltext/S0960-9822(21)01339-7 |
APA Style
Mtenga, A. B., Fimbo, A. M., Shewiyo, D. H., Mwambene, S. J., Kasekwa, E. E., et al. (2025). Efficacy of Antifungal Medicines Against Clinical Isolates of Candida Species Responsible for Vaginal Candidiasis from Regional Referral Hospitals in Tanzania. American Journal of Life Sciences, 13(6), 198-207. https://doi.org/10.11648/j.ajls.20251306.13
ACS Style
Mtenga, A. B.; Fimbo, A. M.; Shewiyo, D. H.; Mwambene, S. J.; Kasekwa, E. E., et al. Efficacy of Antifungal Medicines Against Clinical Isolates of Candida Species Responsible for Vaginal Candidiasis from Regional Referral Hospitals in Tanzania. Am. J. Life Sci. 2025, 13(6), 198-207. doi: 10.11648/j.ajls.20251306.13
AMA Style
Mtenga AB, Fimbo AM, Shewiyo DH, Mwambene SJ, Kasekwa EE, et al. Efficacy of Antifungal Medicines Against Clinical Isolates of Candida Species Responsible for Vaginal Candidiasis from Regional Referral Hospitals in Tanzania. Am J Life Sci. 2025;13(6):198-207. doi: 10.11648/j.ajls.20251306.13
@article{10.11648/j.ajls.20251306.13,
author = {Adelard Bartholomew Mtenga and Adam Mitangu Fimbo and Danstan Hipolite Shewiyo and Saxon Joseph Mwambene and Elizabeth Erasto Kasekwa and Revocatus Evarist Makonope and Shaban Bikiz Kombo},
title = {Efficacy of Antifungal Medicines Against Clinical Isolates of Candida Species Responsible for Vaginal Candidiasis from Regional Referral Hospitals in Tanzania},
journal = {American Journal of Life Sciences},
volume = {13},
number = {6},
pages = {198-207},
doi = {10.11648/j.ajls.20251306.13},
url = {https://doi.org/10.11648/j.ajls.20251306.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajls.20251306.13},
abstract = {Vaginal candidiasis, caused by Candida species affects a significant proportion of women worldwide. Although different antifungal medicines are being used to treat the infection, the emergence of resistance against these medicines have been reported. This study assessed the efficacy of antifungal medicines which are recommended for treatment in the Tanzania Standard Treatment Guidelines against clinical isolates of Candida spp. Presumptive Isolates of Candida spp. collected from Regional Referral Hospitals (RRH) were transported to the Tanzania Medicine and Medical Devices Authority (TMDA) Microbiology laboratory for identification and confirmation by PCR. The confirmed isolates were used for susceptibility testing to establish the efficacy of antifungal medicines. Results indicate that Candida albicans (54%) was the most prevalent Candida spp. among isolates collected. Among the antifungal medicines tested, Miconazole showed the highest efficacy against 229 isolates of Candida spp. with 89.2% of the isolates being susceptible. This was followed by Clotrimazole, with 79.9% and Nystatin, 79.5% of isolates were susceptible, while Voriconazole showed moderate efficacy with 68.9%. Fluconazole demonstrated the lowest efficacy among the tested antifungals with 63.3%. Both Candida albicans and non-albicans Candida spp. displayed similar susceptibility patterns. Out of the 229 Candida spp. isolates tested, 4.4% were found to exhibit multidrug resistance. Findings from this study suggest that despite the observed resistance, the majority of antifungal medicines listed in the Standard Treatment Guidelines in Tanzania remain effective and are still considered reliable for treating vaginal candidiasis.},
year = {2025}
}
TY - JOUR T1 - Efficacy of Antifungal Medicines Against Clinical Isolates of Candida Species Responsible for Vaginal Candidiasis from Regional Referral Hospitals in Tanzania AU - Adelard Bartholomew Mtenga AU - Adam Mitangu Fimbo AU - Danstan Hipolite Shewiyo AU - Saxon Joseph Mwambene AU - Elizabeth Erasto Kasekwa AU - Revocatus Evarist Makonope AU - Shaban Bikiz Kombo Y1 - 2025/12/09 PY - 2025 N1 - https://doi.org/10.11648/j.ajls.20251306.13 DO - 10.11648/j.ajls.20251306.13 T2 - American Journal of Life Sciences JF - American Journal of Life Sciences JO - American Journal of Life Sciences SP - 198 EP - 207 PB - Science Publishing Group SN - 2328-5737 UR - https://doi.org/10.11648/j.ajls.20251306.13 AB - Vaginal candidiasis, caused by Candida species affects a significant proportion of women worldwide. Although different antifungal medicines are being used to treat the infection, the emergence of resistance against these medicines have been reported. This study assessed the efficacy of antifungal medicines which are recommended for treatment in the Tanzania Standard Treatment Guidelines against clinical isolates of Candida spp. Presumptive Isolates of Candida spp. collected from Regional Referral Hospitals (RRH) were transported to the Tanzania Medicine and Medical Devices Authority (TMDA) Microbiology laboratory for identification and confirmation by PCR. The confirmed isolates were used for susceptibility testing to establish the efficacy of antifungal medicines. Results indicate that Candida albicans (54%) was the most prevalent Candida spp. among isolates collected. Among the antifungal medicines tested, Miconazole showed the highest efficacy against 229 isolates of Candida spp. with 89.2% of the isolates being susceptible. This was followed by Clotrimazole, with 79.9% and Nystatin, 79.5% of isolates were susceptible, while Voriconazole showed moderate efficacy with 68.9%. Fluconazole demonstrated the lowest efficacy among the tested antifungals with 63.3%. Both Candida albicans and non-albicans Candida spp. displayed similar susceptibility patterns. Out of the 229 Candida spp. isolates tested, 4.4% were found to exhibit multidrug resistance. Findings from this study suggest that despite the observed resistance, the majority of antifungal medicines listed in the Standard Treatment Guidelines in Tanzania remain effective and are still considered reliable for treating vaginal candidiasis. VL - 13 IS - 6 ER -
Tanzania Medicines and Medical Devices Authority (TMDA), Dar es Salaam, Tanzania;Department of Pharmaceutical Microbiology,Muhimbili University of Health and Allied Sciences (MUHAS), Dar es Salaam, Tanzania
Tanzania Medicines and Medical Devices Authority (TMDA), Dar es Salaam, Tanzania
Tanzania Medicines and Medical Devices Authority (TMDA), Dar es Salaam, Tanzania
Tanzania Medicines and Medical Devices Authority (TMDA), Dar es Salaam, Tanzania
Tanzania Medicines and Medical Devices Authority (TMDA), Dar es Salaam, Tanzania
Tanzania Medicines and Medical Devices Authority (TMDA), Dar es Salaam, Tanzania
Tanzania Medicines and Medical Devices Authority (TMDA), Dar es Salaam, Tanzania
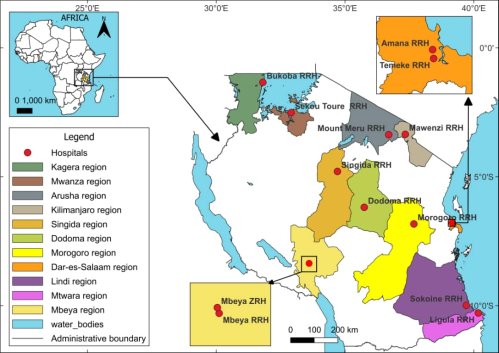
Figure 1. Map of Tanzania showing coverage of regions for sample collection.
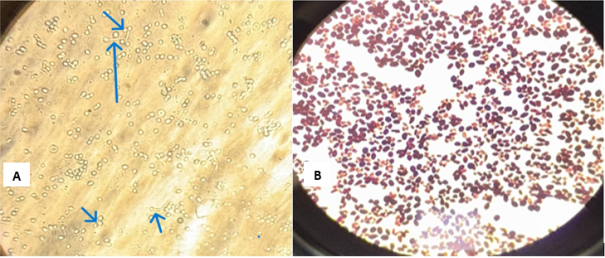
Figure 2. Microscopic identification of Candida spp. using wet mount image (A) and Gram staining image (B).
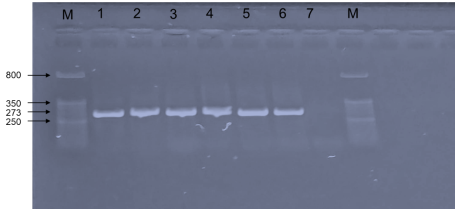
Figure 3. Gel electrophoresis image of PCR product of CalB gene (273 bp) for identification of C. albicans, whereby Lane M marker, Lane 1 Standard C. albicans ATCC 10231 (positive control) Lane 2-6 positive samples of C. albicans isolates, Lane 7 negative control.
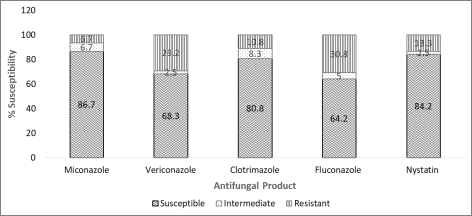
Figure 4. Susceptibility Profile of Candida albicans Isolates to Commonly Used Antifungals.

